
The results from the present study support IXE effectiveness in the management of PsA in a real-world setting, with rapid and sustained improvements across key disease domains. Highly encouraging findings were also observed for DRR over a 24-month period of treatment, regardless of patients clinical and treatment variables.
The clinical characteristics of PsA in our cohort largely align with the existing literature, especially considering the reported wide variability in the manifestations of dactylitis, enthesitis, and axial involvement22,23,24,25. The high prevalence of overweight and obesity, as highlighted by BMI values, was expected26. Obesity is one of the most common comorbidities in PsA, supporting the theory that adipose tissue plays a role not only in metabolic processes but also in inflammatory and autoimmune mechanisms.
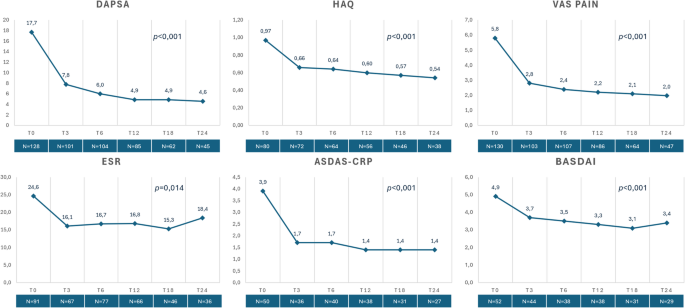
Concerning clinical effectiveness, IXE treatment allowed a steady disease control across all disease domains in our patients, with a rapid onset of response, observed at 3 months and maintained thereafter. In fact, we registered a considerable reduction in key clinimetric indexes, including DAPSA, ASDAS-CRP and BASDAI. These improvements were most notable in both peripheral and axial joint symptoms. Additionally, a similar trend was observed in the MDA composite score, reflecting significant progress not only in joint involvement but also in skin symptoms and enthesitis (VLDA reached by 16% of patients at T24 and MDA by 34% of patients).
Such data are especially important since, despite the inclusion of PsA patients in various real-world cohort studies involving IXE, specific PsA-related efficacy outcomes (beyond the PASI score used for the assessment of PsO) have been analyzed to a limited extent14,27,28,29,30,31,32,33. In particular, it is worth mentioning the results from a 2024 multicentric prospective registry analysis from the Gruppo Italiano Studio Early Arthritis (GISEA) collecting 223 PsA patients. The authors reported a significant improvement within 6 months of IXE treatment for TJC and SJC and DAPSA score, persisting up to 24 months14.
Other recent real-world reports have further contributed to the evidence on IXE, although with different target populations and study objectives. Building on this context, our findings extend the existing real-world literature on IXE in two main ways. Chiricozzi et al. (LOTIXE) evaluated long-term IXE effectiveness in moderate-to-severe plaque PsO, primarily using dermatologic endpoints (e.g., PASI and DLQI) in a responder-enriched population requiring ≥ 12 months of continuous treatment30, whereas our study focuses on a CASPAR-classified PsA cohort and evaluates longitudinal musculoskeletal disease activity with validated disease activity indexes (e.g., DAPSA) together with PROs and functional measures. Furthermore, Bellis et al. investigated IXE drug survival and predictors of discontinuation in a monocentric PsA cohort focusing on DRR12, while our multicenter dataset integrates both multi-domain effectiveness trajectories and 24-month treatment persistence, including patients who discontinued during follow-up, thereby reflecting routine rheumatology practice closely.
Furthermore, a notable finding in our group was the favorable impact of IXE on QoL, as measured by the HAQ score, which is of particular importance given the well-documented disease burden associated with PsA7,34,35. IXE also significantly reduced pain, as demonstrated by changes in the VAS score. This is a critical finding, given that pain is a predominant symptom in PsA, and its control is essential for effective disease management. There is growing evidence of central sensitization mechanisms leading to chronic pain in patients with PsO and PsA36. Indeed, we recorded a substantial prevalence of 17.6% of fibromyalgia in our cohort. Considering the involvement of IL-17 in neuroinflammation and neuropathic pain, anti-IL-17 therapies, including IXE, have been hypothesized to play a role in modulating chronic pain, supported by encouraging preclinical results37. However, these mechanistic considerations are speculative and cannot be inferred from the present observational data.
More than half of the patients in our cohort had already been treated with b/tsDMARDs, a substantial proportion of whom had used anti-TNF. Indeed, a detailed subgroup analysis of both patient groups showed no significant differences in DRR achievement based on the type of previously administered biologic drug, nor was there an overall reduction in DRR compared to biologic-naïve patients. This observation is consistent with other available studies, although real-world data suggest that biologic-naïve patients may experience slightly greater efficacy, albeit with minimal differences from pre-treated patients7,31. The overall evidence thus offers reassuring support for the effective and lasting use of IXE even in later lines of therapy in PsA.
A considerable portion of our cohort had axial involvement. In those patients ASDAS-CRP and BASDAI scores decreased over follow-up, which was associated with improvement in axial disease activity measures in this observational setting. This finding is particularly notable given the limited data on IL-17 inhibitors in psoriatic spondylarthritis38. It is becoming increasingly evident that radiographic(r)-axSpA and psoriatic axSpA represent distinct pathophysiological entities24,39. This distinction highlights the need for dedicated research into psoriatic axSpA, rather than relying on data extrapolated from studies on non r- and r-axSpA. Furthermore, ASDAS-CRP and BASDAI are validated for axSpA rather than axial PsA, and their use in axial PsA should be interpreted cautiously.
Most patients remained on IXE throughout the observation period, with a high persistence rate of 73.3% at the 24-month follow-up. Treatment discontinuation was primarily due to primary or secondary inefficacy, followed by mild AEs such as injection site reactions or non-severe infections. Overall, IXE was shown to be safe and well-suited for long-term treatment. Real-world data from insurance claims databases and cohort/registry studies on patients with PsO, PsA, and axSpA reported IXE treatment persistence rates exceeding 70%, with follow-up periods extending up to 24 months40,41,42,43, with overall superiority in retention rates compared to other biologics (except ustekinumab)44,45,46. Two recent studies evaluating IXE use in PsA patients reported DRR of 43.8% at 38 months and 57% at two years, with similar proportions of discontinuation due to inefficacy or mild AEs12,13. Braña et al. identified depression and prior methotrexate use as predictors of treatment discontinuation13.
In our cohort, women had a significantly lower DRR compared to men, although no differences were observed based on axial involvement, prior biologic exposure, or BMI class. This finding is consistent with other studies, which have shown that women with PsA generally report worse patient-reported outcomes (PROs) related to quality of life, fatigue, and pain, and have less favorable responses to biologic treatment compared to men47. Interestingly, although a recent pooled data analysis on the phase 3 SPIRIT-P1 and SPIRIT-P2 RCTs highlighted higher DAPSA improvements in males48, attributable to a greater therapeutic effect in this sex, Chimenti et al. found IXE to be equally effective in both sexes after 24 months14,48. This discrepancy could be possibly attributed to the increased pain sensitivity and risk for clinical pain observed among women compared to men49, as well as the higher prevalence of fibromyalgia in the female population50, which may contribute to a greater persistence of symptoms in women, even after treatment and despite the achievement of remission or improvement in disease manifestations. Studies specifically designed on PsA patients with concomitant fibromyalgia could help clarify these intriguing aspects.
Furthermore, the lack of correlation between BMI values and the efficacy of IXE treatment is not unexpected, as previous studies have reported similar findings consistent with other anti-IL-17 therapies51,52. Conversely with other classes of biologic drugs, such as anti-TNF, where body weight has been shown to significantly impact treatment outcomes52,53. This observation holds great significance in highlighting the remarkable versatility of IXE treatment, especially in terms of providing a personalized therapy for PsA patients, tailored not only to their specific clinical presentation but also to their unique comorbidity profile.
Regarding the potential impact of psoriasis on IXE effectiveness and long-term drug survival, no clinically meaningful differences were observed in our cohort. Disease activity, as assessed by DAPSA, improved consistently in patients both with and without psoriasis at baseline. Moreover, a significant impact of skin involvement on DRR was not demonstrated; this analysis was limited by marked group imbalance and a low number of events, which reduced statistical power and resulted in unstable survival estimates.
The proportion of patients who discontinued treatment due to AEs was consistent with findings in the literature, with no severe AEs reported7. Indeed, injection site reactions and non-severe infections, especially localized candidiasis, have been previously described in clinical trials and real-world studies11,54.
Although our data on gastrointestinal involvement is limited due to missing information, in the two patients with CD, IXE did not lead to disease exacerbation, despite previous reports suggesting a potential risk for disease activation, likely related to the crucial role of IL-17 signaling in maintaining intestinal epithelial barrier integrity55,56,57.
The relevance of the findings from our study is supported by its multicentric design and quite large sample size, making it one of the most comprehensive real-world studies on IXE in PsA to date. Furthermore, the detailed evaluation of treatment efficacy across multiple disease domains, including the MDA criteria, provides further valuable insights. The extended follow-up period also strengthens our data, offering a clearer picture of IXE long-term performance. Lastly, the inclusion of a substantial number of patients with psoriatic axSpA, a clinically distinct entity from r-axSpA, adds to the novelty of our findings, contributing to the limited data available on IL-17 inhibitors in this context. Nevertheless, these results should be interpreted with caution, as disease activity was assessed using ASDAS-CRP and BASDAI, indices originally developed and validated for axSpA rather than specifically for psoriatic axSpA.
Our study is limited by its observational and retrospective design, which offers less robust evidence compared to interventional studies and limits causal inference, particularly in the absence of a comparator group. The retrospective design may introduce selection bias potentially influencing both treatment response and retention. Additionally, there was missing data for some variables (e.g., nail psoriasis), and outcome availability decreased over time, which may bias longitudinal estimates. Despite this limitation, the consistency of improvement across multiple disease activity indices, patient-reported outcomes, and inflammatory markers, along with sensitivity analyses results, support the robustness of the observed treatment effect.