
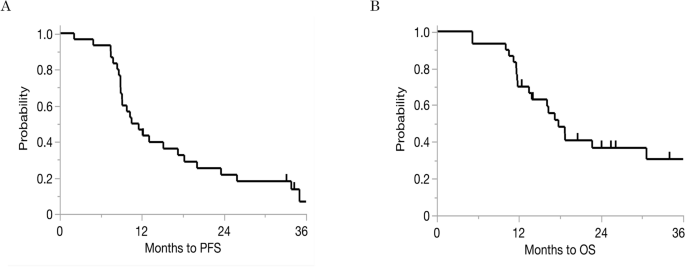
Our previous study demonstrated that intraperitoneal paclitaxel improves survival outcomes in patients with gastric cancer and peritoneal metastasis9,10,11,12,13,20. Furthermore, the median survival time for patients treated with systemic chemotherapy alone has been reported as 12.5 months21. However, this study found that intraperitoneal paclitaxel therapy achieved a median survival time of 17.8 months (with a median follow-up of 16.7 months, ranging from 4.9 to 48.8 months). This suggests a clinically relevant advantage.
Paclitaxel, a taxane-based chemotherapeutic agent, induces cytotoxicity by inhibiting microtubule depolymerization. This arrests the cell cycle and promotes cell death when paclitaxel is administered systemically22. However, when administered intraperitoneally, paclitaxel achieves sustained high concentrations and remains in the peritoneal cavity for an extended period owing to its lipophilicity and high molecular weight, which restrict peritoneal clearance9.
High-dose paclitaxel–induced immunogenic cell death (ICD) has been reported to enhance memory T cell responses by releasing damage-associated molecular patterns (e.g., HSPs, HMGB1, and ATP) that promote dendritic cell maturation and tumor antigen presentation23,24,25,26.
Our findings suggest that intraperitoneal paclitaxel may beneficially modulate the peritoneal immune microenvironment, thereby enhancing anti-tumor immunity and contributing to improved clinical outcomes. Despite the potential of immunotherapy to enhance anti-tumor immune responses, not all patients respond well to intraperitoneal paclitaxel. This discrepancy may result from immune escape mechanisms such as the increased presence of regulatory immune cells and immune checkpoint molecules, which suppress effective anti-tumor responses and counteract the immunostimulatory effects of ICD.
Our previous study demonstrated that high-dose paclitaxel triggers apoptosis based on morphological analysis. Recent evidence suggests that immunogenic cell death (ICD) — a regulated form of cell death capable of eliciting an adaptive immune response — can arise from various modalities of cell death, including apoptosis, necroptosis, and ferroptosis27. Thus, the paclitaxel-induced apoptosis observed in our previous study may represent an immunogenic variant of regulated cell death that contributes to antitumor immune activation.
This study demonstrated that the immune composition of ascitic fluid is associated with clinical outcomes in patients with gastric cancer and peritoneal metastasis receiving intraperitoneal paclitaxel. Notably, elevated levels of CD4+ T cells and CD19+ B cells, as well as increased expression of FOXP3 and CTLA-4, were associated with worse survival outcomes based on Kaplan–Meier analysis. Moreover, Ridge regression analysis further highlighted CD4+ T cells and CTLA-4 as key contributors to poor 1-year prognosis, suggesting the central role of regulatory T cell-mediated immunosuppression. In contrast, a higher proportion of NKT-like cells was associated with improved PFS in Kaplan–Meier analysis, and this finding remained significant in both univariable and multivariable models. NK cells emerged as the most favorable factor in the multivariable Ridge model, indicating their potentially dominant role in antitumor immunity when multiple immune parameters are considered simultaneously.
The observed association between elevated CD4+ T cells and poorer outcomes likely reflects regulatory T cell expansion, as evidenced by high FOXP3 and CTLA-4 expression28.
The correlation heatmap revealed that CD4+ T cells exhibited moderate positive correlations with FOXP3 (ρ = 0.49) and weaker positive correlations with CTLA-4 (ρ = 0.35). These findings suggest that a significant portion of CD4+ T cells are immunosuppressive regulatory T cells. Conversely, CD8+ T cells demonstrated strong negative correlations with CD4+ T cells (ρ = −0.62), FOXP3 (ρ = −0.45), and CTLA-4 (ρ = −0.32). This suggests that, in environments dominated by regulatory T cells, the activity of cytotoxic T cells may be suppressed.
Regulatory T cells suppress the function of effector T cells through the secretion of IL-10 and the competitive inhibition of co-stimulatory signaling via CTLA-429,30. These findings emphasize the importance of regulatory T cell-mediated immunosuppression in drug resistance29,31,32. In accordance with these mechanisms, recent studies have reported that the development of peritoneal metastases fosters an immunosuppressive intraperitoneal environment. This environment is characterized by reduced cytotoxic T-cell activity and overall attenuation of antitumor immune responses33.
Importantly, while NKT-like cells showed a consistent trend toward improved outcomes, NK cells emerged as the strongest favorable factor for 1-year PFS in the Ridge regression analysis. This finding contrasts with the Kaplan–Meier analysis, which did not demonstrate a significant prognostic impact of NK cells. Notably, NK cells exhibited consistently low correlation coefficients with all other immune parameters in the correlation heatmap. This apparent statistical independence suggests that NK cells may exert distinct and autonomous effects within the peritoneal immune microenvironment. Such independence may explain why NK cells emerged as the most favorable prognostic factor in the multivariable Ridge model, despite their lack of significance in univariable and Kaplan–Meier analyses.
Natural killer T (NKT) cells exhibit direct anti-tumor activity and, upon activation via dendritic cell antigen presentation, secrete interferon gamma, thereby promoting the activation of cytotoxic T lymphocytes and NK cells34,35,36. Although NKT cells represent less than 0.1% of peripheral T cells, they are relatively abundant in tissues such as the liver and omentum, where they can account for up to 10% of T cells37,38,39. Notably, omental NKT cells have specific cytotoxicity against CD1d-expressing tumor cells, and elevated CD1d expression has been reported in gastric cancer40,41. These findings suggest that NKT cells may play a key role in anti-tumor immunity within the peritoneal cavity. In our study, we evaluated NKT-like cells (CD3+CD56+, with no CD1d restriction confirmed) as a surrogate population, and their depletion was associated with poor prognosis, possibly reflecting immune exhaustion or tumor-mediated suppression.
Previous studies have reported favorable prognostic associations with NK cell infiltration in primary gastric tumors, but their functional status may vary depending on the microenvironment. In malignant ascites, NK cell counts reportedly decrease in patients with peritoneal dissemination16. Furthermore, analyses of NK cell subsets in ovarian cancer have shown that CD56brightCD16− NK cells, which have a high capacity to produce cytokines, are associated with better outcomes, whereas CD56dimCD16+ NK cells demonstrate lower cytotoxicity and lack prognostic relevance42,43,44. Our study did not include NK cell subset analysis, so further research is needed to clarify their role in malignant ascites.
Increased B cell levels were also linked to worse clinical outcomes. Although B cells may have tumor-suppressive roles, regulatory B cells can promote immunosuppression via the secretion of cytokines (e.g., IL-10, IL-35, and TGF-β) and by enhancing regulatory T cell proliferation45,46,47. Prior studies in ovarian cancer have implicated ascitic regulatory B cells in disease progression48,49 and our results suggest a similar mechanism may apply in gastric cancer with peritoneal metastasis. However, in our Ridge regression model, B cells had a weak positive coefficient for 1-year PFS, implying a potential prognostic benefit when accounting for multiple immune parameters.
This discrepancy between the univariable/Kaplan–Meier results and the Ridge model highlight the heterogeneous nature of B cells. Further analyses of B cell subsets, including regulatory versus effector phenotypes, are warranted to clarify their distinct prognostic roles within the peritoneal immune environment.
In this cohort, PD-L1 expression was uniformly low in ascitic cell block specimens and showed no association with survival (CPS: no cases ≥5; PFS: p=0.344; OS: p=0.934).
This likely reflects the low intrinsic PD-L1 expression of peritoneal metastases. However, technical factors may have also contributed50. The 28-8 antibody clone was used on cytology-derived cell blocks. Pre-analytical conditions and inter-assay variability among commonly used clones (e.g., 28-8, 22C3, SP142, and SP263) can reduce staining sensitivity, leading to lower CPS values51. Further consideration will be required in the future.
Collectively, these findings suggest that pre-treatment immune profiling of ascitic fluid may be useful to inform prognosis and guide therapeutic selection. Kaplan–Meier analysis identified high CD4+ T cell and B cell counts and reduced NKT-like cell levels as unfavorable factors, and multivariable Ridge regression analysis further underscored the prognostic significance of CD4+ T cells and NK cells. These results highlight the importance of evaluating immune subsets in combination, rather than in isolation. Patients with immunosuppressive profiles—such as those with elevated regulatory cell populations or diminished cytotoxic effectors—may derive limited benefit from intraperitoneal paclitaxel therapy and could be candidates for immunomodulatory combination approaches, including those incorporating anti–CTLA-4 agents or regulatory T cell/regulatory B cell depletion strategies.
This study has several limitations. First, the relatively small sample size and single-center design may limit the generalizability of our findings. Although clinical variables such as age and PCI score may influence immune composition, they were not included in the multivariable model because of the limited sample size, to avoid overfitting. Instead, Ridge regression was applied to mitigate estimation bias and multicollinearity, allowing a stable evaluation of the relative contribution of immune parameters to prognosis. Future large-scale multicenter studies should incorporate these clinical factors to validate the independent prognostic significance of intraperitoneal immune markers.
Second, although our analysis included major immune cell subsets, we did not perform functional assays or subset analyses of NK and B cells. Further studies characterizing CD56bright versus CD56dim NK cells and regulatory B cells would enhance understanding of their roles in the peritoneal immune environment. Third, immune profiling was limited to pretreatment ascitic fluid. Longitudinal sampling during and after therapy could provide insights into dynamic treatment-induced immune modulation. Despite these limitations, our findings underscore the potential of immune profiling of ascitic fluid as a non-invasive strategy to predict response to intraperitoneal chemotherapy and to inform future combination approaches targeting immune suppression.
The intraperitoneal immune microenvironment plays a pivotal role in determining responses to intraperitoneal chemotherapy in patients with gastric cancer and peritoneal metastasis. High CD4+ T cell and B cell counts and FOXP3 and CTLA-4 expression are associated with poor prognosis. In contrast, higher NKT-like cell levels correlate with improved PFS. Furthermore, multivariable Ridge regression analysis identified high CD4+ T cell and CTLA-4+ cell levels as the strongest unfavorable predictors of 1-year PFS, whereas NK cells emerged as the most favorable independent prognostic factor. These findings suggest that immune profiling of ascitic fluid may serve as a valuable prognostic tool for predicting therapeutic efficacy and guiding treatment selection, particularly in identifying patients who may benefit from combination strategies that target immune suppression.