
Study design
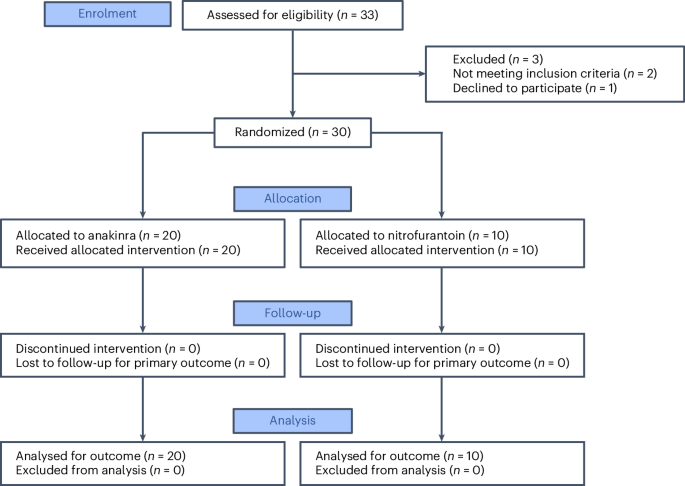
For this randomized, open-label, single-centre, phase 2 trial, patients were enrolled at the Clinic for Urology, Pediatric Urology and Andrology in Giessen, Germany. The trial was registered on 27 July 2021 at the German Clinical Trials Register number DRKS00025964 (https://drks.de/search/en/trial/DRKS00025964) and EudraCT number 2019-004209-28. Diagnosis and treatment followed an established clinical pathway, and mandated routine tests included urinalysis, full blood count, and urine and blood sampling for molecular analyses (Fig. 2a). No formal sample size calculation evaluating the power of the trial has been performed. However, consideration regarding the sample size was made based on previous studies of anakinra in a murine acute cystitis model2,5. A total of 33 women were invited to participate in the study, but 3 were not enrolled as they did not fulfil the inclusion criteria, resulting in a study cohort of 30 participants; 20 participants were treated with anakinra and 10 participants with nitrofurantoin (Fig. 1).
The trial was conducted in accordance with the principles of the Declaration of Helsinki, the International Council for Harmonisation guidelines for good clinical practice, and applicable national laws and regulatory requirements. Ethical approval was obtained from the German Ethical Review Authority (ethics vote AZ10/21). Written information was presented to the patients, and participation required a signed informed consent.
Patients
Female adult patients with an acute episode of recurrent uncomplicated cystitis were included in this study (Table 1). Enrolment was based on a sum score of the main UTI symptoms at visit 1 ≥ 6 as reported on the ACSS typical domain7,14,15,24,25. The ACSS is a self-reporting questionnaire for the clinical diagnosis of acute uncomplicated cystitis7,14 and is also a proven instrument for patient-reported outcome assessment25,26. The ACSS method (see questionnaire in Supplementary Fig. 1, http://ACSS.world) has been developed as a diagnostic tool for uncomplicated UTI, to more precisely define patients with this disease state based on reported outcome measurement26. It has been tested in trials comparing antibiotic versus non-antibiotic therapy, in which effects on clinical criteria are important as main objectives15.
The typical symptom score cut-off ≥6 was used as a symptomatic inclusion parameter. Typical symptoms include frequency, urgency, burning pain at urination, incomplete bladder emptying, lower pelvic pain and haematuria; each symptom is evaluated according to a predefined Likert scale7 (intensity score 0–3 and a maximum total score of 18). Typical symptoms must be acute, developed within ≤6 days of enrolment, and the patients must have a history of recurrent cystitis (≥3 documented episodes in the past year or ≥2 documented episodes in the past 6 months). Follow-up visits were performed on days 2, 5, 15 and 30 and after 6 months.
Inclusion and exclusion criteria stated in the protocol are as follows:
Inclusion criteria
-
Stable patients with an acute episode of recurrent uncomplicated cystitis
-
Sum score of the typical UTI symptoms at visit 1 ≥6, reported on the ACSS; urgency; frequency; burning at voiding; feeling of incomplete emptying; lower abdomen pain; blood in urine
-
Typical symptoms acute, developed within ≤6 days
-
History of recurrent cystitis (≥3 documented episodes in the history in the past year or ≥2 documented episodes in the history in the past 6 months)
-
Female participants, 18–65 years old
-
Signed written informed consent form
-
Capability and willingness to comply with study procedures
-
Negative urine pregnancy test in women of childbearing potential
-
Contraception
Exclusion criteria
-
Breastfeeding
-
Signs of pyelonephritis
-
Uncontrolled diabetes mellitus
-
Neutropenia (<1.5 × 109 l−1)
-
Signs of genital infections (vaginitis, cervicitis)
-
Anamnestic exclusion of patients with active severe infections, history of viral hepatitis
-
Patients using Cytochrome P450 medications (for example, warfarin, phenytoin)
-
Patients using phenytoin medication
-
Extragenital conditions, nephrological conditions, urological conditions, urinary catheters that may lead to complicated UTI
-
Severe uncontrolled systemic disease
-
Systemic antibiotic therapy within 5 days before inclusion
-
Impaired renal function (creatinine clearance <60 ml min−1)
-
Known allergies or contraindications to Kineret and nitrofurantoin Uro-Tablinen
-
Malign diseases
-
Immunosuppression
-
Previously enrolled in this trial
-
Pathological liver enzymes
-
Polyneuropathies
-
Glucose-6-phosphate dehydrogenase deficiency
-
Participation in other interventional clinical trials
-
Use of diclofenac and ibuprofen analgetic medication while participating in this clinical trial
Trial procedures
All enrolled participants were randomized to two study treatment groups at visit 1; the chance for allocation to the anakinra group or nitrofurantoin group was 2:1. Randomization was performed by the central office of the Center for Clinical Trials of the Philipps-University Marburg. The administrated investigational product was then documented together with the date, time and study code in the source documentation and electronic Case Report Form (eCRF). The analysis of the study parameters was blinded. Patients randomized to anakinra were allocated five prefilled syringes with 100 mg per 0.67 ml solution for injection (Kineret, Sobi), procured from the University Hospital Giessen and Marburg Clinic Pharmacy. Anakinra was administered by subcutaneous injection of 100 mg once a day for 5 days, given at around the same time each day. Patients receiving nitrofurantoin (Uro-Tablinen, Zentiva), procured from the University Hospital Giessen and Marburg Pharmacy Marburg, or with a prescription after 6 July 2023 owing to supply shortage, were instructed to take the drug orally at home on their own twice a day (2 × 100 mg) for 5 days. Proper documentation, including accompanying documents, was used to ensure that the antibiotic nitrofurantoin was used properly.
Outcomes
The overall objective of the trial was to evaluate the efficacy and safety of anakinra for the treatment of acute cystitis, compared with conventional antibiotic treatment with nitrofurantoin, using a randomized protocol.
The primary efficacy end-point was the change in symptom score after 5 days of treatment, measured by the ACSS method.
Safety end-points included change in laboratory safety variables, vital signs, physical examination from baseline and the incidence of adverse events, treatment-emergent adverse events and serious adverse events during the trial.
Secondary end-points were the presence of bacteriuria and leukocyturia at each visit up to week 26 of the study and UTI recurrences up to 6 months.
Exploratory end-points included urine proteomics, gene expression analysis and DNA sequence analysis.
ACSS
The ACSS (see questionnaire in Supplementary Fig. 1, http://ACSS.world) is a patient self-reporting questionnaire consisting of two parts: diagnostic part A and follow-up part B. Part A contains 18 items, allocated to 4 domains: 6 items on typical symptoms of acute cystitis (‘typical’ domain), 4 items for differential diagnosis (‘differential’ domain), 3 items on quality of life (‘QoL’ domain) and 5 items on additional conditions that may affect therapy (‘additional’ domain). Each item of the first three domains (typical, differential and QoL) is fitted with a 4-point Likert-type scale for assessing the severity of each symptom ranging from 0 (no symptom or discomfort) to 3 (severe symptom or discomfort). The ‘additional’ domain contains dichotomous ‘yes or no’ questions. Furthermore, part B includes an additional ‘dynamics’ domain formed by a question about the general evolution and changes in symptoms22.
Urine cultures and tests
Urine samples were analysed by quantitative bacterial cultures and dip slide for haematuria and leukocytes.
Midstream urine samples were cultured on cystine–lactose–electrolyte-deficient agar, Columbia nalidixic acid agar, MacConkey agar and Sabouraud agar (Thermo Fisher). Negative urine was <103 CFU ml−1. Antibacterial resistance of the isolates was identified by automated antimicrobial susceptibility testing (VITEK 2, Biomerieux), followed by disk diffusion test using the European Committee on Antimicrobial Susceptibility Testing (EUCAST) break-point criteria.
Blood samples
Analysis of white blood cell counts, including differential counts, was performed on venipunctured blood samples.
Gene expression analysis
RNA, stabilized and purified from peripheral blood using Tempus blood RNA tubes and a purification kit (Applied Biosystems), was subjected to expression microarray analysis: 10 ng of total RNA was amplified and fragmented using the GeneChip 3′ IVT Pico labelling kit and hybridized onto Human HT Clariom S arrays (all Thermo Fisher Scientific). Samples were processed in the GeneTitan System following the manufacturer’s instruction (Thermo Fisher Scientific). Transcriptomic data were normalized using the robust multi-chip analysis algorithm implemented in the Transcriptome Analysis Console software (TAC v.4.0.1.36, Applied Biosystems, Thermo Fisher Scientific). A probeset (gene) is considered expressed if ≥50% of the samples in the dataset have a gene level detected above background value < 0.05. Fold change was calculated by comparing each treatment group with RNA obtained at the time of diagnosis (day 1). Differentially expressed genes and regulated pathways were analysed using Ingenuity Pathway Analysis software (IPA v.01-23-01, Qiagen).
Statistical analysis
The typical symptoms, quality of life and differential symptoms were analysed using the ordinal logistic mixed-effects model (or cumulative link mixed model) fitted with the Laplace approximation. Typical symptom, quality-of-life and differential symptom score values were used as unstructured thresholds to calculate the cumulative odds ratio, with the assumption of proportional odds across thresholds, and every time point was included as a repeated ordinal outcome. This was followed by estimated marginal mean (or least-squares means) post hoc comparisons with Tukey’s P value adjustment for comparing a family of five estimates, with ordinal dependent variables, repeated measures over time, between-subject factor (treatment) and random effect (subject). Treatment effects between time points within each arm, as well as differences between treatments at each time point, were evaluated (see statistical analysis results in Supplementary Fig. 2).
The symptom dynamics were analysed using the Cochran–Armitage trend test. Values are single ordinal measures of patient-reported outcome, independent of the other scores. Higher numbers mean worsening of symptom outcome compared with enrolment. The anakinra and nitrofurantoin groups were compared for each time point.
Recurrence rates were analysed by Wilcoxon matched-pairs signed rank test for each treatment group and Mann–Whitney test for each time point. Wilcoxon matched-pairs signed rank test was also used for the sub-analysis of patients with ≥105 CFU ml−1 and patients with <105 CFU ml−1, comparing day 1 and day 5.
Relative gene expression was analysed by ANOVA using the empirical Bayes method, and genes with a P value < 0.05 and an absolute fold change >1.5 were considered differentially expressed. P values for enrichment of canonical pathways and diseases and functions were calculated using a right-tailed Fisher’s exact test with a null hypothesis of no non-random association. Activation Z scores were two sided.
For white blood cell counts and differential counts, normal distribution was tested using the D’agostino and Pearson, Anderson–Darling, Shapiro–Wilk and Kolmogorov–Smirnov tests. No complete dataset successfully passed a normality test. Data were therefore analysed using aligned rank transform ANOVA (see statistical analysis results in Supplementary Fig. 2). The aligned rank transform ANOVA model estimated significant changes across time points, which were compared using Wilcoxon matched-pairs signed rank test with the two-stage step-up method of Benjamini, Krieger and Yekutieli FDR (Q) = 1%, with non-parametric data, within-subject fixed effect (time), between-subject fixed effect (treatment) and random-effect intercept (subject).
Statistical analysis was performed using GraphPad Prism version 10.5.0 for macOS or R Studio version 2025.05.01 Build 513 (Posit Software, PBC) and R version 4.5.1 using the code available at Code Ocean (https://doi.org/10.24433/CO.8500789.v1)27.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.